Alan G. Christianson, NMD
Abstract
Whole Body Cryotherapy (WBC) is a hypothermic application designed to reduce musculoskeletal pain and inflammation. WBC stimulates the sympathetic nervous system via alpha-adrenergic receptors, causing dramatic peripheral vasoconstriction. This induces adaptive changes correlating with effects of analgesia, reduction of inflammation, and increases in serum markers of tissue repair.
Research conducted over the last two decades, primarily in Europe, has established therapeutic efficacy of WBC in a wide range of clinical areas. The largest focuses of research have been pain management and athletic performance. It has been shown to effectively reduce pain and swelling and improve physical performance. Due to the numerous adaptive physiological responses, WBC has also been studied as an adjunct treatment for: atopic dermatitis, cardiovascular health, depression and Multiple Sclerosis.
Introduction
WBC utilizes the analgesic and therapeutic effects of cold water and ice, and greatly increases the beneficial effects while reducing the discomfort and treatment durations. It originated in Japan in the early 1970’s and is currently in use worldwide.
Countries using Whole Body Cryotherapy
- United States
- United Kingdom
- France
- Italy
- Turkey
- Slovenia
- Czech Republic
- Hungary
- Romania
- Moldova
- Russia
- Belarus
- Ukraine
- Kazakhstan
- Qatar
- Australia
- Canada
The first demonstration unit installed in the US was April 2009. The first commercial unit went in place February 2010. WBC became a media topic in early 2011 due its successful implementation by the Nike athletes under coach Alberto Salazaar. It gained national attention when positively featured on the Dr. Oz show in March of 2011. At the time of this writing, approximately 25 units are now in operation in America. The users include professional sports teams, athletic trainers, pain management clinics and med-spas. (Antra Getzoff of Millennium ICE, personal communication January 20, 2012)
This article is to serve as an introduction to WBC and to review pertinent literature demonstrating its therapeutic effects.
History
 Local hypothermic applications in the forms of water, ice and snow have been used throughout recorded history as means of reducing pain. Until the recent past, mechanisms of analgesia were poorly understood. As an extension of research meant to elucidate the analgesic effects of hypothermia, Whole Body Cryotherapy (WBC) was developed.
Local hypothermic applications in the forms of water, ice and snow have been used throughout recorded history as means of reducing pain. Until the recent past, mechanisms of analgesia were poorly understood. As an extension of research meant to elucidate the analgesic effects of hypothermia, Whole Body Cryotherapy (WBC) was developed.
In the 1970’s, the work of Dr. Yamaguchi et. al. showed that the benefits of cold did not relate to chilling the underlying tissues. Rather the benefits correlated with the chilling of superficial peripheral afferent nerves known as thermoreceptors. The most systemic benefits were found to occur when the thermoreceptors were chilled quickly and to a great degree1.
He set out to find a method to quickly cool the largest possible amount of skin in the briefest
amount of time without causing the cold to penetrate. Numerous trials of various methods led him to the use of brief exposures to gasiform liquid nitrogen in dried air.
Normally the thermoreceptors operate at the ambient temperature of peripheral skin, roughly 90°F. Immersion in ice cold water has the capacity to lower thermoreceptors to roughly 59°F after 300 seconds of exposure. Most find this painful and hard to tolerate. WBC has the capacity to lower thermoreceptors to 30-32°F in 30 seconds with minimal penetration and therefor much less discomfort.
Pioneering studies showed that treatments shorter than 4 minutes would yield no tissue trauma or frostbite and treatments over 3 minutes yielded no additional therapeutic effect1. Because of this, WBC treatments range from 2.5 – 3 minutes in duration.
Typical Treatment Session
WBC treatments work by subjecting the patient’s skin to controlled levels of gasiform liquid nitrogen. The treatment is conducted in a device called a cryochamber. Before treatment, the cryochamber is pre-cooled and dried, and the patient is given informed consent. Next, the patient disrobes inside the chamber, keeping on socks to protect their toes. Men also wear regular underwear to protect external genitalia. The floor of the unit elevates allowing the patient’s head to be outside of the chamber so they can continue to breath room air.
Nitrogen gas is safe to breathe since it makes up roughly 80% of our atmosphere, however in a pure state it displaces oxygen. The patient’s fingertips are protected by keeping their hands placed on a padded ledge around the top of the chamber.
During a session, bursts of nitrogen are circulated around the chamber, directed away from the patients skin. The bursts serve to maintain the therapeutic temperature. In a typical 3 minute session, 10 second bursts are released with 20-30 second pauses between them. The ambient temperature in the chamber is maintained at -200 to -250°F throughout the course of treatment.
Ideal treatment intensities cause a spontaneous shiver reflex to began just at the end of the session. The cryotherapist is able to adjust certain variables, to achieve a brief shiver reflex without the cold being too intense. These include: amount of pre-cooling, duration of bursts, duration of pause between bursts and the duration of the session.
Those who are older, less physically active and less tolerant of cold, can achieve this response with milder treatments and briefer durations. Those who undergo a series of treatments usually prefer colder treatments as their series progresses.
Immediately after the 2.5 – 3 minute session, the majority of subjects experience marked improvements in pain and joint discomfort and notice measurable reductions in joint edema. Most also experience endorphin releases normally experienced only after intense exercise.
Mechanisms of Action
The genome of modem humans experienced the majority of its evolution over the Pleistocene Epoch. This time period is demarcated by alternating glacial (ice ages) and interglacial (temperate) periods. The majority of time was likely spent in glacial periods, thus engendering many genetic adaptations to cold.2
These adaptations are the likely reason that WBC induces homeostatic responses from most of the body’s regulatory mechanisms.
The initial cold startle response elicits a strong sympathetic nervous system reaction. This causes a dramatic parasympathetic rebound.3,4
The circulatory system undergoes dramatic peripheral vasoconstriction followed by strong rebound vasodilation. This improves peripheral vascular tone while reducing histamine release due to vascular permeability.4
The neuromuscular system responds with a decrease in troponin I, creatine kinase and edema.5
Positive immune responses include increased white blood cell counts, increased anti-inflammatory cytokines, and reduced pro-inflammatory prostaglandin PGE2.6,7
In the endocrine system, WBC triggers an increase in noradrenaline, P-endorphins, adrenocorticotropic hormone(ACTH) and pro-opiomelanocortin (POMC) concentrations.8
Therapeutic Applications – Multiple Controlled Studies
Pain – Arthritis
Arthritis, including rheumatoid arthritis (RA) and other rheumatic conditions (AORC), are the leading cause of disability in the United States.9 Reducing these symptoms, thereby enabling patients to engage in necessary weight-bearing exercise, protects patients from further degeneration.
A study conducted at the Institute of Rheumatology in Warsaw compared the outcomes of 40 patients with rheumatoid arthritis divided to receive WBC or Physical Therapy daily for 4 weeks. Outcomes tracked were blood markers of inflammation and patient reported pain scores.
Histamine levels were considerably lower in the blood of patients with RA following WBC and remained lower over a period of at least three months after treatments were discontinued.
Those receiving WBC were also shown to have a therapeutic down-regulation of polymorphonuclear cells and coupled with an up-regulation of calprotectin levels and sodium potassium ATPase activity.
No significant changes in histamine levels or the other biochemical parameters were measured in groups of patients treated only with Physical Therapy.
Most importantly, pain scores were significantly diminished and reduced more than they did in those receiving Physical Therapy only.
Therefore, WBC can play an integral role in diminishing symptoms of RA. Figure 1 illustrates the significant drop in patient pain score with and without WBC.10
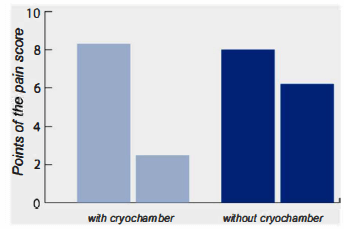
Figure 1: Number of Swollen Joints in Patients with Rheumatic Arthritis11
Pain – Fibromyalgia
Fibromyalgia (FM) is characterized by chronic inflammation, accompanied by widespread muscle pain and pressure-sensitive tender points. In addition to reducing pain, WBC may effectively diminish other symptoms of fibromyalgia including sleep disturbances, fatigue, depression and anxiety, cognitive difficulties and headaches.12
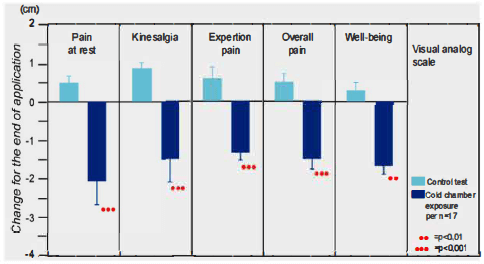
Forty-two patients with fibromyalgia, who satisfied the diagnostic standards of the American College of Rheumatology, were assessed for pain (O= no pain, 10 = worst pain). Additional measures included levels of creactive protein (CRP), morning stiffuess and number of swollen joints. After 10 daily WBC sessions, amelioration of pain at rest, pain on movement (kinesalgia) and exertion pain, improved by 12 to 21 % on pain scale scores by those treated, as opposed to the control group, which showed no significant changes.
The study also found a reduction in the number of painful pressure points in the treated group, and a reduction in the need for analgesics by 30 percent compared to the control group.13 Based on these findings, WBC in treating symptoms of fibromyalgia may be optimized at early onset, or acute stages of the disease.
Figure 2 illustrates the significant reduction in FM patient pain score reports with and without WBC.
Figure 2: WBC Effects on Symptoms ofFibromyalgia14
Pain – Anklyosing Spondylitis
WBC can considerably improve functional capacity and quality of life in patients suffering from ankylosing spondylitis (AS). Fricke et al. measured disease activity in 20 AS patients receiving inpatient treatment involving daily physiotherapy and WBC exposure for a 28 day period. Their outcomes were contrasted with control subjects who received physiotherapy without WBC.
Measured parameters included range of motion, mobility of individual vertebral regions, rate of erythrocyte sedimentation and hemoglobin values. Those treated with WBC showed significant improvements (p=0.0009, p=0.0196).
After 28 days of therapy, both groups showed a statistically significant decrease of the disease activity
(p=0.0001, p=0.0050). However, the only improvement reported in the control group was improved function in the thoracic spine (p=0.0235), whereas the group undergoing daily WBC presented a statistically significant improvement ( p=0.0002 ) of subjective complaints (morning stiffness, abnormal fatigue, joint pain as well as subjective discomfort) and functional improvements in all 3 vertebral regions.(p=0.003, p=0.0019, p=0.0124).15
Athletics – Inflammation
Ice plunges have long been used for decades for exertional pain and are an expected fixture in athletic training rooms. Consequentially, athletes have easily taken to the idea of WBC as an improvement on the ice plunge. The benefits appear to be greater, while the treatment duration and discomfort is less. WBC may enhance performance via adaptations in cardiovascular function, muscle and motor unit activation, enhanced muscular perfusion and optimization of muscle metabolism.16 Reduced symptoms of sport-induced hemolysis following WBC have also been documented.17-21
In a study published in July of 2011, a group of researchers set up an experiment to determine the changes WBC may have on markers of exercise-induced muscle damage and inflammation in a simulated trail running race. A group of 11 male endurance athletes completed two trials separated by a 1 month wash out. One trial included daily cryotherapy sessions daily for 4 days after the exertion. The event consisted of a 48 minute variable effort on treadmills meant to simulate rolling hills.
Measured markers included interleukins 1,6 and 10, tumor necrosis factor alpha, c-reactive protein and white blood count. Measurements were taking pre exercise, immediately post and at 24, 48, 72 and 96 hour intervals.
Those receiving WBC showed enhanced muscular recovery via a significant reduction in the inflammatory process. These benefits manifested with immediate post-exertional inflammation as well as later onset inflammation.22
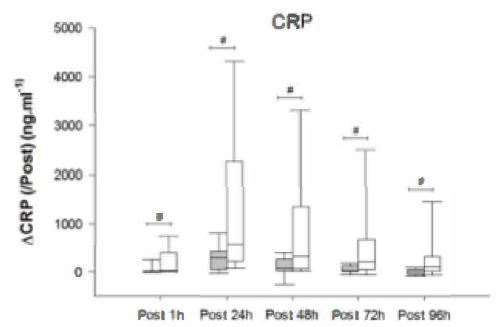
Figure 3: CRP Levels in WBC athletes (shaded) vs control group (unshaded) 22
Athletics – Immune Function
Several studies indicate the possible immuno-modulating effects of WBC. Many athletes involved in rigorous training are at risk for exercise induced anemia. Banfi et al 2009 found increased haptoglobin concentrations (56.6 mg/L to 75.2 mg/L; p<0.05) and mean cell volume( MCV)(84.6 fL to 87.6 fL) following five WBC sessions in ten male rugby players. They also found that when hematocrit was unmodified, hemoglobin concentrations were significantly reduced.23
In a related study, fifteen young, clinically healthy men underwent ten sessions of WBC. Measurements were taken of white blood cell count, level ofIL6 and the total oxidative and antioxidative status. Post WBC treatments, the men showed a significant increase in white blood cell count (lymphocytes and monocytes) and levels of interleukin 6 with one treatment, with peak levels following the full course.24
Athletics – Anaerobic Performance
A 2009 study published in the Journal of Thermal Biology demonstrated enhanced neuromuscular performance during a drop-jump exercise, as well as maximal voluntary contraction (MVC) force of the wrist flexors following WBC (-110 °C, 3 times/week for 3 months)25
A separate study determined the influence ofWBC on anaerobic capacity. In it, 30 subjects performed two ergocycle trials before and after a course often WBC sessions while monitoring power output in watts.
Decreased time to reach peak power (6.67 to 5.92 seconds) was observed post-WBC in males. Data indicated an increase in maximal anaerobic power (11.1 to 11.9 Watts x weight in kg-1 ), a marked (P<0.05) increase in mean power (723.9 vs. 756.1 Watts) and an increase in total work (13.77 vs. 14.53 kiloJoules).26
Therapeutic Applications – Preliminary Research
Atopic Dermatitis
Researchers with the Skin and Allergy Hospital in Helsinki used whole-body cryotherapy for 18 adults with atopic dermatitis three times a week for 4 weeks, followed by an 8-week follow-up period. Adjunctive treatments were all discontinued during the trial.
The final scoring showed a significant decrease from an index symptom score of 38.7 to 31.1. 27
Cardiovascular System – Heart Rate Variability
WBC has been shown to induce cardiac parasympathetic modulation similar to that achieved with prolonged exercise training. They both lower the sympathetic nervous system’s effect on heart rate variability.27
Cardiovascular Health – Lipids
Polish researchers showed that lipid panels could be improved with WBC sessions in a dose dependent response. Optimal outcomes were achieved with 20 daily treatments.28
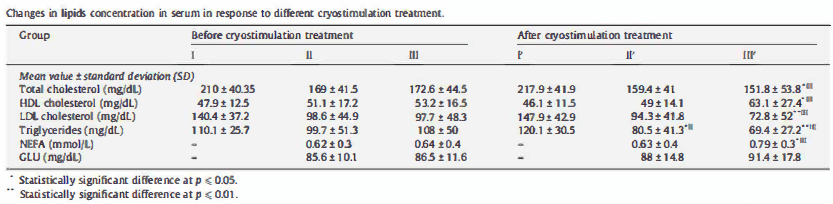
Figure 4 Changes in serum lipid concentrations. Group I received 5 treatments, group II received 10 and group III receive 20.28
Depression and Anxiety
A 2008 study published in the Archives of Immunology and Experimental Therapy utilized the Hamilton’s depression rating scale (HDRS) and Hamilton’s anxiety rating scale (HARS) to determine the efficacy of WBC as a short term-adjunct treatment for depression, mood and anxiety disorders. After 3 weeks of daily WBC treatments, at least a 50% reduction in depressive symptoms was observed in 34.6%, compared to 2.9% in the control group. Anxiety was also alleviated by at least 50% in 46.2% of the WBC group with no significant changes in control group.29
Multiple Sclerosis
Multiple sclerosis (MS) is a variably progressive disease characterized by immune-mediated inflammatory reactions as well as neurodegeneration and depression.20 Neutralizing oxidative stress may serve as a useful approach to protect patients with MS from further neurological harm. A preliminary study conducted in 2010 compare changes in total oxidative status and activities of chosen endogenous anti-oxidant enzymes in erythrocytes of patients with MS before and after WBC against those of a control group.45 Thirty-two patients with MS had ten sessions of WBC in conjunction with exercises. The control MS group (n=16) had only exercises. Levels of Total Antioxidative Status (TAS) in MS patients were distinctly reduced compared to healthy subjects.30
Case Studies
Following are several typical case reports from WBC users. They are meant to illustrate results expected from the literature and also show insights on other conditions WBC may benefit.
Rheumatoid Arthritis/Fibromyalgia
Case 1 is a 60 year old female with a 15 year history of debilitating pain from both rheumatoid arthritis and fibromyalgia. She is additionally diagnosed with Chronic Fatigue Immuno Deficiency Syndrome. Her normal subjective pain scores ranged from 8-10. She received a course of 15 WBC treatments of 3 minutes at -200°F. During this time she did not engage in physical therapy or other new interventions. Since unsuccessfully trying many medication combinations, she was on no pain medicines during her WBC treatment. After the first session, the patient noticed a significant reduction in joint pain, greater joint mobility and improved energy levels. These results were reported consistently throughout the course of treatments. She did notice the most pronounced benefits when treatments were done with less time in between. During treatment, her subjective pain scores came down to an average of 2-3 which had not been the case for over 15 years.
Migraines
Case 2 is a 40 year old male with a history of chronic migraines for 10 years. Typically he experienced 2-3 migraines per month, each lasting 3-5 days. He received little benefit from prophylactic or abortive medications, both conventional and natural. The patient read about WBC and was informed that little published data existed on it benefitting migraines, but anecdotally, many of our patients did find it helpful. On the day of his first treatment, the patient presented with an acute migraine which had already been present for 2 days. Roughly 2 minutes after his initial treatment of 3 minutes at -200°F, his migraine intensity reduced by 90%. Two hours after treatment, his headache was resolved. He has since completed 4 weekly WBC treatments and seen only 1 minor migraine start but not manifest during the month of treatment.
Post-surgical rehabilitation
Case 3 is a 38 yr old male who underwent total knee replacement 4 weeks prior. He was experiencing significant swelling and redness of his joint and was unable to complete physical therapy exercises properly. After a single treatment of 3 minutes at -200°F, his knee swelling reduced by 3 inches. The following day, he was able to complete his exercises and his physical therapist said his range of motion improved to that of a typical patient 6-8 weeks post surgery.
Knee replacement ( 4 weeks post-op)
Degenerative disc disease
Case 4 is a 41 year old male who gives the following testimonial:
“I have suffered from a degenerative disc between C-5 and C-6 of my spine. I have tried physical therapy, chiropractic treatment, and even considered surgery. Prior to Cryotherapy, I managed my pain with ibuprofen several times a day. My day to day pain level ranged from 6-9 (on a scale of 1 to 10 where 10 is the worst). After about 4 treatments my pain dropped to about 4 after 10 treatments my day to day pain level hovers around 1-2. I was skeptical in the beginning, wondering about placebo effects, etc… But I am now convinced there is a physiological effect from my treatments.
In addition to a significant reduction in my chronic pain, I have experienced the following:
- Blood pressure decease. My original readings were 126/86 and now are 116/70.
- My resting heart rate has dropped from 63 bpm to about 48 bpm.
- I have lost 8 lbs
- My endurance has increased dramatically.
- I have effectively fought off the colds and flu brought home from pre-school by my children”
Contraindications
Healthy subjects can experience a transitory increase of systolic and diastolic blood pressure of 10 points as treatment starts. Labile hypertension, unstable angina, recent myocardial infarction, congestive heart failure and end stage renal failure are therefore contraindications.
Raynaud’s syndrome and ‘cold allergy’ are contraindicated due to risk of topical vaso-constrictive reactions.
Pregnant women and children under age 10 are recommended to avoid treatment as well as anyone mentally unable to properly follow procedural instructions. Children under the age of 18 are recommended to have treatment only with parental guidance and consent.
Adverse events
After decades of use, WBC has had no complications when protocols have been followed. Cases of frostbite have occurred when patients wore removable jewelry, removed protective socks or exceeded recommended durations of treatment. Cases have been reported of hypoxic fainting when patients attempted to breathe the pure nitrogen gas.
Conclusions
Whole Body Cryotherapy has been documented to safely and quickly benefit chronic pain and inflammation. It also has an established role in benefitting athletic performance.
Due to its It is homeostatic inducing effects on a myriad of body symptoms and preliminary evidence, it may also have a role in benefitting cardiovascular function, mood disorders and neurodegenerative states.
Given the diverse plausible benefits, tolerability, safety and brief duration of treatments, promising opportunities exist for further studies in these areas.
Footnotes:
- Yamauchi T, Kim S, Nogami S. Extreme cold treatment(-150 °C) on the whole body in rheumatoid arthritis X. Europaischer Kongress fur Rheumatologie Abstract band. 1981; 1054.
- P. Gibbard and T. Van Kolfschoten. The Pleistocene and Holocene Epochs, ch. 22, in F. M. Gradstein et al. A Geologic Time Scale (2004), Cambridge University Press.
- Marino F, Sockler JM, Fry JM. Thermoregulatory, metabolic and sympathoadrenal responses to repeated brief exposure to cold. Scandinavian journal of clinical and laboratory investigation. 1998;58(7):537-545.
- Kargus DK, Lum KB, Auber TT, et al. Studies on Whole-body Cryotherapy. Pain. 1999:1-32.
- Westerlund T, Oksa J, Smolander J, et al. Neuromuscular adaptation after repeated exposure to whole-body cryotherapy (-110 °C). Journal of Thermal Biology. 2009;34(5):226-231.
- Banfi G, Melegati G, Barassi A, et al. Effects of the whole-body cryotherapy on NTproBNP, hsCRP and troponin I in athletes. Journal of Science and Medicine in Sport. 2009;12(6):609-610.
- Lubkowska A, Szygula Z, Klimek AJ, et al. Do sessions of cryostimulation have influence on white blood cell count, level of IL6 and total oxidative and antioxidative status in healthy men? European Journal of Applied Physiology. 2010;109(1):67-72.
- Leppaluoto J, Westerlund T, Huttunen P, et al. Effects of long-term whole-body cold exposures on plasma concentrations of ACTH, beta-endorphin, cortisol, catecholamines and cytokines in healthy females. Scandinavian journal of clinical and laboratory investigation. 2008;68(2): 145-153.
- Anon. Rheumatoid Arthritis. Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion. 2011. Available at: http://www.cdc.gov/arthritis/basics/rheumatoid.htm. Accessed December 13, 2011
- Ibid Kargus
- Ibid
- Anon. Fibromyalgia. Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion. 2011. Available at: http://www.cdc.gov/arthritis/basics/fibromyalgia.htm. Accessed December 13, 2011.
- Offenbacher M, Stucki G. Physical therapy in the treatment of fibromyalgia. Scandinavian journal of rheumatology Supplement. 2000;113:78-85.
- Gutenbrunner C, Englert G, Neues-Lahusen M, et al. Analgetic effects of natural sulphur baths and coldchamber expositions in Fibbromyalgia. Phys Rehab Kur Med 1999;9:56 ± 62.
- Senne B, G, Maier C, Wittenberg H. et al. Effects of whole-body cold chamber in patients with ankylosing spondylitis. Presented to the University Hospital of the Ruhr-University Bochum 1/24/2001.
- Westerlund T, Oksa J, Smolander J, et al. Neuromuscular adaptation after repeated exposure to whole-body cryotherapy (-110 °C). Journal of Thermal Biology. 2009;34(5):226-231.
- Banfi G, Krajewska M, Melegati G, et al. Effects of the whole body cryotherapy on haematological values in athletes. British Journal of Sports Medicine. 2008;(December).
- Dugue B, Smolander J, Westerlund T, et al. Acute and long-term effects of winter swimming and wholebody cryotherapy on plasma antioxidative capacity in healthy women. Scandinavian journal of clinical and laboratory investigation. 2005;65(5):395-402.
- Lubkowska A, Szygula Z, Klimek AJ, et al. Do sessions of cryostimulation have influence on white blood cell count, level ofIL6 and total oxidative and antioxidative status in healthy men? European Journal of Applied Physiology. 2010;109(1):67-72.
- Lubkowska A, Chudecka M, Klimek A, et al. Acute effect of a single whole-body cryostimulation on prooxidant-antioxidant balance in blood of healthy, young men. Journal of Thermal Biology. 2008;33(8):464- 467.
- Pournot H, Bieuzen F, Louis J, et al. Time-Course of Changes in Inflammatory Response after Whole-Body Cryotherapy Multi Exposures following Severe Exercise. Lucia A, ed. PLoS ONE. 2011;6(7):8.
- Banfi G, Lombardi G, Colombini A, et al. Whole-body cryotherapy in athletes. Sports Medicine.
2010;40(6):509-517. - Lubkowska A, Szygula Z, Klimek AJ, et al. Do sessions of cryostimulation have influence on white blood cell count, level ofIL6 and total oxidative and antioxidative status in healthy men? European Journal of Applied Physiology. 2010;109(1):67-72.
- Ibid Westerlund
- Klimek AT, Lubkowska A, Szygula Z, et al. Influence of the ten sessions of the whole body cryostimulation on aerobic and anaerobic capacity. International journal of occupational medicine and environmental health. 2010;23(2): 181-189.
- Wozniak A, Wozniak B, Drewa G, et al. The effect of whole-body cryostimulation on the prooxidantantioxidant balance in blood of elite kayakers after training. European Journal of Applied Physiology.
2007; 101(5):533-537. - Westerlund T, Uusitalo A. Heart rate variability in women exposed to very cold air (-110°C) during wholebody cryotherapy. J Therm Biol. 2006; 31 :342-346.
- Lubkowska A, Banfi G, Dolegowska B, et al. Changes in lipid profile in response to three different protocols of whole-body cryostimulation treatments. Cryobiology 61 (1) p. 22-26.
- Rymaszewska J, Ramsey D, Chladzinska-Kiejna S. Whole-body cryotherapy as adjunct treatment of depressive and anxiety disorders. Archivum Immunologiae et Therapiae Experimentalis. 2008;56(1):63-68.
- Miller E, Mrowicka M, Malinowska K, et al. Effects of whole-body cryotherapy on a total antioxidative status and activities of antioxidative enzymes in blood of depressive multiple sclerosis patients. The world journal of biological psychiatry the official journal of the World Federation of Societies of Biological Psychiatry. 2011;12(3):223-227.